October is ADHD awareness month! I actually learned very little about ADHD’s effects on communication as a graduate student and it wasn’t until I began seeing lots of patients with ADHD that I started to wonder about the connection between the disorder and speech and langauge. Since then I’ve had the opportunity to work with psychologists and occupational therapists who know far more about the disorder than I do as well as dozens of kids, colleagues, and friends who have taught me so much about their own struggles with ADHD.
ADHD & Communication
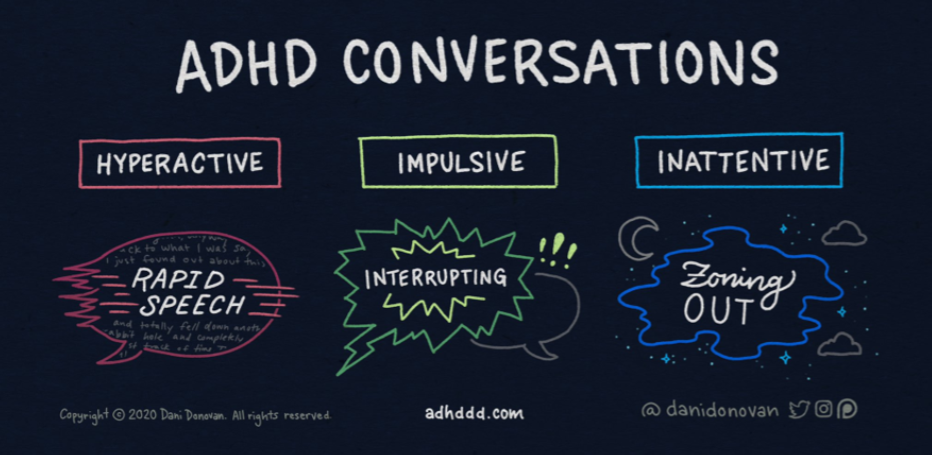
ADHD effects communication greatly. Children with ADHD are more likely than the general population to struggle with pronunciation (phonological disorder), narrative retell (receptive-expressive langauge disorder), using grammatical features (expressive langauge disorder), and social skills (pragmatic langauge disorder). Here are some ways ADHD affects communication skills:
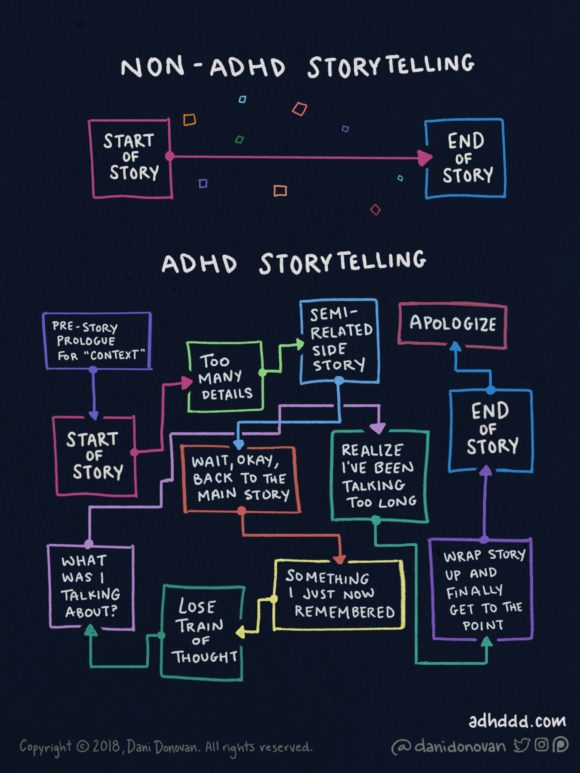
- ADHD significantly affects narrative retell and narratives of children with ADHD are characterized by disorganization (events told out of sequence), decreased details, decrease cohesion, and decreased accuracy.
- ADHD also affects pragmatic language/social skills, which is unsurprising for those of us who know children who have ADHD are often too distracted to pick up on social cues or maintain topics and too impulsive to maintain expected physical distance or wait their turn during conversation.
- ADHD affects language memory, which means children with ADHD often have trouble following directions and using age-expected grammatical features such as irregular past-tense verbs for children who are 4 or older.
- ADHD is often comorbid with phonological disorder.
- Children with ADHD are at greater risk for langauge disorders.
ADHD Misconceptions
As a provider I’ve come into contact with a lot of misconceptions about ADHD. I’ll address the ones that bother me the most…
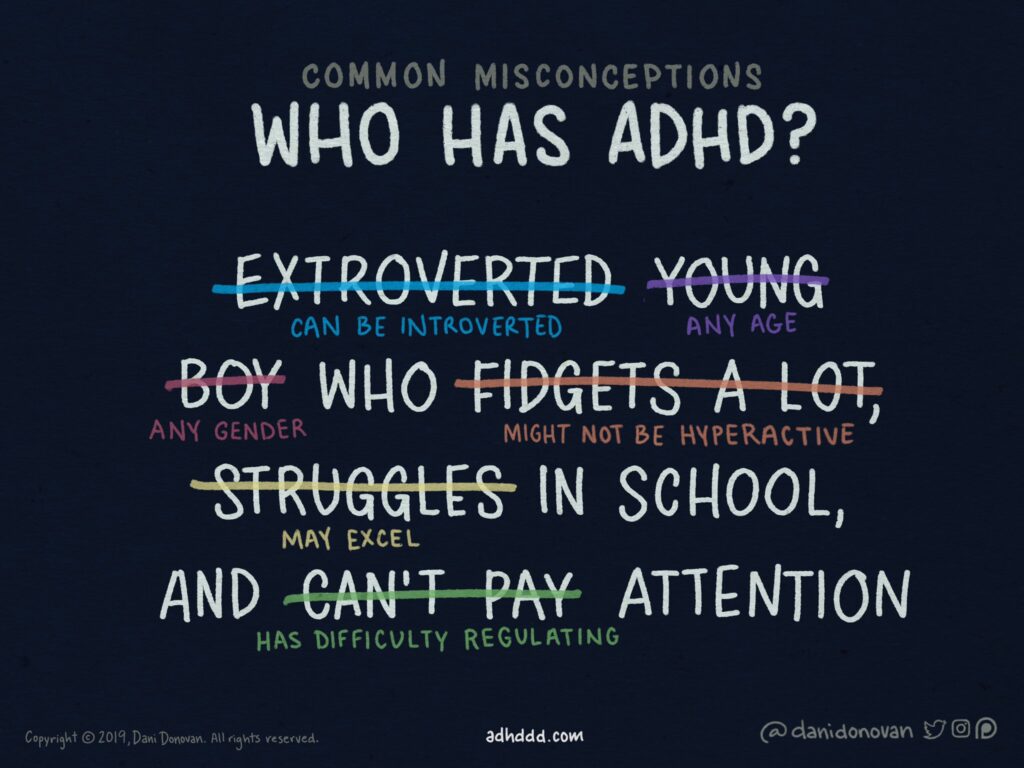
- Children who have ADHD are often capable of extremally focused attention on their interests. This is actually a symptom of ADHD and is called “hyper-focus.” “Attention deficit” doesn’t mean they cant focus at all – it means they can’t modulate their focus like the rest of us.
- Children who have ADHD aren’t always hyper. The correct acronym is actually “AD/HD” because children either have “inattentive type” or “hyperactive type” ADHD. Children and adults with the inattentive of ADHD might seem more “tired” or low-energy than the general public.
- Sensory impairment is not a characteristic of Autism Spectrum Disorder (ASD) alone. I’ve heard various people say that because a child has a sensory impairment they must have ASD, but sensory impairment is also a characteristic of ADHD. I find that the best way to draw a line between ASD and ADHD is, instead, impulsivity, which is rarely seen outside ADHD in school-aged children. That being said, I’ve seen a couple children who have both ADHD and ASD and it’s sometimes very difficult to tell whether a child’s social skill deficits are being caused by one or the other (or both!).
- Showing a child with ADHD your annoyance and anger is not helpful for them. Due to their impulsiveness, they’re often as annoyed by their own behavior as us around them. Snapping at, glaring at, or raising your voice with a child who has ADHD only makes them feel worse for the behaviors that are out of their control and doing so regularly can make them feel discouraged. Instead, try to give yourself compassion as you maintain as neutral a tone and facial expression as possible while addressing behaviors caused by ADHD. I also find that talking to the child about the behaviors that annoy me helps both of us. For example, I talk to kids about how “I need to watch your hands more. Do you find that your hands do things without you even realizing what they’re doing? I need to be more careful about putting away the things we both don’t want your hands touching.”
- Medications for ADHD actually don’t increase a child’s likelihood of developing addictions. In fact, the opposite is true. Adults with ADHD who didn’t receive medication in childhood are actually more likely to develop addictions than their peers with ADHD who experienced medication in their youth. This is because those who don’t experience the benefits of medication often “self-medicate” through illicit substances. This is especially important since addicts seeking recover have a higher rate of ADHD than the general population (30% compared to 10%).
- Children don’t usually grow out of ADHD. In fact, many “grow into” it, instead. This means it’s usually less obvious in adults, but these adults spend massive amounts of energy to appear as “neuro-typical” as they do. Getting through a work day can be 10 times as taxing on them as it is for the rest of us.
Modifications to Treatment Techniques
As SLPs, many of the features of ADHD such as impulsivity and sensory regulation are outside of our scope of practice. However, these deficits often interfere with our treatment of the language memory, expressive langauge, receptive langauge, pragmatic langauge (social skills), and articulation/phonology that are in our scope. So while I use the same treatment techniques with kids who have ADHD as those who don’t I also add in lots of modifications for those who need it (regardless of an ADHD diagnosis). Here are some of my favorites for ADHD:
- Environmental Modification – This is a fancy way of saying “design your room to minimize distractions.” I set up my office so my computer is not visible from the treatment area and I even have a privacy screen I can pull in front of it if I need to. I have covers for my toy shelves and I keep the boardgames for older kids on the top (where little ones can’t reach them). I keep all scissors, permanent markers, and glue stashed near my computer where kids can’t get to them.
- Regulation Tools – Many children who have ADHD are either over-reactive or under-reactive to parts of their environment. The patients I work with who have ADHD usually favor sitting/bounding on a yoga ball, sitting on a wiggle cushion, or having a lap buddy while we work on our speech and language. The Zones of Regulation curriculum is also really helpful for these kids.
- VARIETY – The ADHD brain thrives on novelty. I try to vary the activities I use for each goal so that we don’t use the same activity more than 2 weeks in a row.
- Choices – This helps increase novelty, too. I let children choose which activities we do while working on their goals and/or which order we do them in. I usually give kids 3 options for each goal. For example, when working on articulation the child can choose from cards, a video game, or a spinner.
- Incorporating Interests – Since children with ADHD have an easier time focusing on their interests I build their interests into therapy activities. For example, for a child who loves Minecraft we can work on their narrative creation/sentence grammar tasks while they make a story about Minecraft using this FREE Minecraft Create-A-Story slideshow.
- Visual Timers – Many people with ADHD experience “time blindness.” This means they experience the passage of time differently than the rest of us. I suspect this is linked to their ability to hyperfocus on interests (which makes time pass extremely fast for them) and their difficulty focusing on other tasks (which makes time pass extremely slow for them). When time can feel so different no wonder they have difficulty learning time and transitioning! I use this visual timer for young children and either this one or this one for school-aged kids.
- Visual Schedules – I’ve been using the Kids ToDo List app for my visual schedule these days. The kids love that the stars jump when they touch them and they get a fish for our ocean when they’re done. Kids can also choose which order they do their activities in because the stars don’t need to be touched in order from top to bottom (changing the order of activities increases the novelty of them even if they’re the same activities).
- Positive Reinforcement – I find positive reinforcement very helpful for kids with ADHD. This can be as simple as giving them praise for doing things they should while ignoring the things they shouldn’t and as advanced as a token economy system. My older patients who have ADHD earn 100 points every appointment if they do all their work (and I divide the points up between the activities) and they can save those points to earn a ticket for various things such as our local natural history museum (1,000 points), Meow Wolf (3,500 points), or even an escape room (25,000 points).
Treating Language Memory
One of the unique features of ADHD on language is it’s effect on langauge memory. This can be measured using the Clinical Evaluation of Langauge Fundamentals, Fifth Edition (CELF-5), Language Memory Index and it’s not uncommon for me to see children with a diagnosis of ADHD who score in the average range for the Core Language, Expressive Langauge, and Receptive Language Indexes, but below this range for the Language Memory Index. When I first started seeing this I was at a loss of what to do, especially since language memory can depend on so many factors such as whether the words to be remembered are related and whether there’s background noise when they’re said. For this I turned to Webber® HearBuilder® and have found so much success with the program that other professionals who share my patients have approached me asking what I did that worked so well. The program automatically considers things such as whether words are related, whether they have visual supports, whether there’s a delay between the words and the child’s response, and whether there’s background noise or even movements to increase distractions. As my patients progress through the Auditory Memory program I notice improvements in their abilities to follow directions, answer questions, retell stories, and converse.
Originally published: 10/01/2022
Want more ideas? Subscribe to my monthly newsletter!